Improving cardiovascular disease prediction with lipoprotein(a)
- Post by: Peter Willeit
- October 2, 2019
- Comments off
Lipoprotein(a) [Lp(a)] is a causal risk factor for cardiovascular disease. In this paper published in JACC we aimed to investigate whether Lp(a) modifies clinical risk assessment in the general community. We measured Lp(a) in 826 men and women (age range, 45 to 84 years) and recorded incidence of cardiovascular diseases over 15 years of follow-up.
In models adjusted for Framingham Risk Score (FRS) and Reynolds Risk Score (RRS) variables, the hazard ratio (HR) for incident cardiovascular disease was 1.37 per 1-SD higher Lp(a) level (SD = 32 mg/dl) and 2.37 when comparing the top fifth quintile with other quintiles. When we added Lp(a) to the RRS, the C-index increased by 0.016.
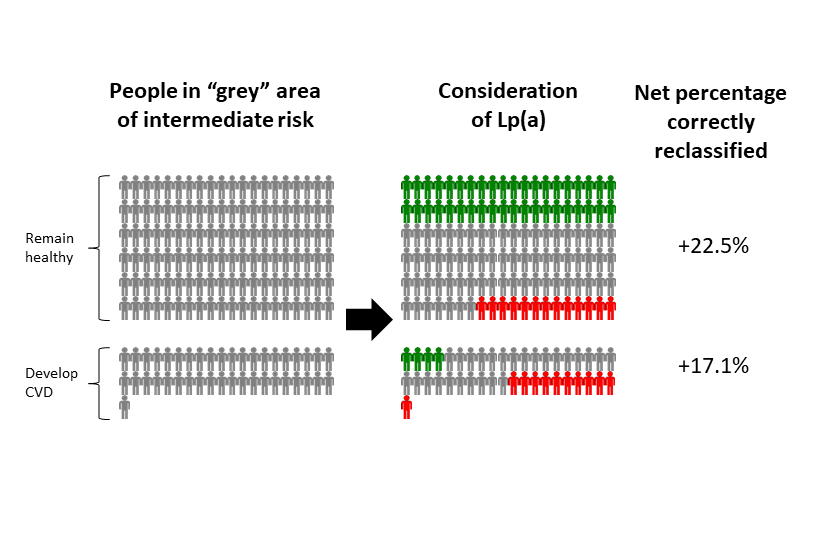
As the next step in our analysis, we evaluated benefits for risk reclassification. Of the 502 subjects who remained free of cardiovascular disease, 82 were correctly reclassified to a lower risk category and 49 were reclassified to a higher risk category (predicted 15-year categories: <7.5%, 7.5% to <15%, 15% to <30%, ≥30%) (p<0.001). Of the 148 subjects who developed cardiovascular disease , 18 were correctly reclassified to a higher risk category and 17 were reclassified to a lower risk category. In subjects at intermediate risk (15% to <30%), the net reclassification improvement afforded by Lp(a) was 22.5% for noncases, 17.1% for cases, and 39.6% overall. Allele-specific Lp(a) levels did not add to the predictive ability of the FRS or RRS or to Lp(a).
Based on these findings we concluded that elevated Lp(a) predicts 15-year cardiovascular disease outcomes and improves cardiovascular risk prediction. The findings suggest that Lp(a) levels may be used in risk assessment of subjects in the general community, particularly in intermediate-risk groups.
The full paper is available at http://dx.doi.org/10.1016/j.jacc.2014.03.061